Purpose of running this test:
The Organics Acid (Nutritional) test (formerly known as the Metabolic Analysis Profile) gives information about intermediates in a number of biochemical pathways in your body. Important methylation cycle markers such as FIGLU, a marker for folate, and methylmalonic acid, a marker for B12, are included in this test.
Additionally, the Organics Acid (Nutritional) test gives information about the turnover and/or breakdown products of several neurotransmitters, including serotonin and dopamine. These are useful in conjunction with neurotransmitter testing to determine the causes of problems such as mood instability, depression, obsessive compulsive disorder (OCD), or the need for nutritional neurotransmitter support.
The Organics Acid (Nutritional) test also generates data about critical energy intermediates and your mitochondrial function. Mitochondrial disorder is being recognized as a factor in the declining health of increasing numbers of both adults and children. Organics Acid (Nutritional) testing is useful for assessing the level of mitochondrial energy intermediates including intermediates in the mitochondrial Krebs cycle. Oxalate is part of the Krebs energy cycle along with other compounds such as malate and fumarate.
In conjunction with a Comprehensive Stool Analysis Test and GI test, the Organics Acid (Nutritional) test can reveal problems with the breakdown of fats in your body and show intermediates that indicate ketosis. In addition, these three tests contain information about bacterial or yeast infestations or infections.
In general, the Organics Acid (Nutritional) test helps you determine areas you need to focus on for additional testing and/or treatment. As noted in the ‘related tests’ section below, high values for specific intermediates on this test help you target which additional tests and/or supplementation may be needed.
| Marker | This table contains the rationale behind my suggestions. These suggestions are for your consideration. Defer your choices to your own health care practitioner, as always. |
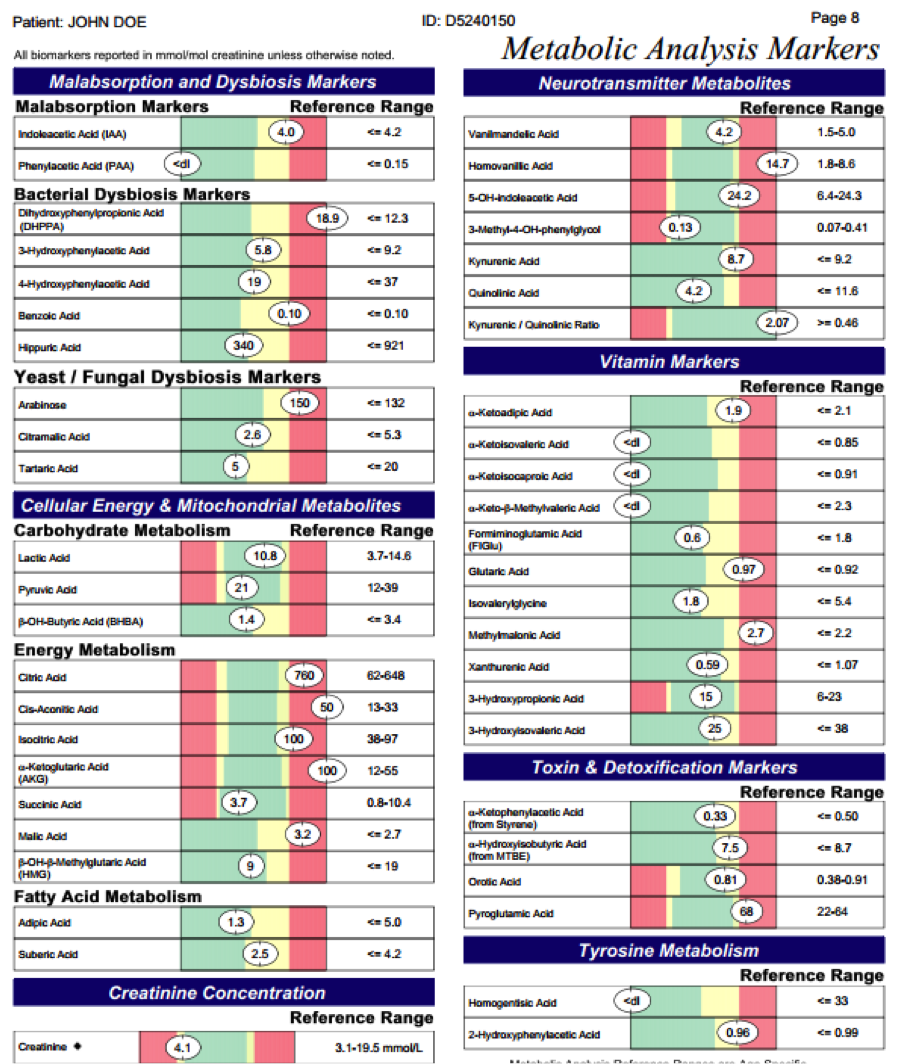
| Indoleacetic acid | An increased indoleacetic acid marker can be due to bacterial breakdown of unabsorbed tryptophan. This may be due to lack of BH4 which converts tryptophan to serotonin, or a need for vitamin B3 (niacin) that helps to process tryptophan. There are several forms of B3, and supplementing with a variety of types of B3 may be helpful. Also, rule out bacterial issues as a cause of high indoleacetic acid. You can use Niacinamide and/or NADH, MTHFR A1298C Liver Support capsules, or Ultimate B Complex. Depending on your levels of hippuric or benzoic acids, and the levels of tyrosine, tryptophan, and/or phenylalanine on a UAA test, as well as aluminum on HMT and/or UEE , you can consider using BH4. Run a CSA test and GI Test to look for bacterial issues. |
| Phenylacetic acid | Phenylacetic acid is formed from bacterial degradation of phenylalanine. Phenylalanine is processed by BH4. So, a lack of BH4, excessive bacteria in your GI tract, excessive ingestion of NutraSweet, supplementation of phenylalanine, or aluminum in your system which impairs BH4 formation, may cause this marker to be high. MTHFR A1298C Liver Support capsules and MetalAway can be used to support natural BH4, as well as to help with aluminum in your system. Depending on your levels of hippuric or benzoic acids, and the levels of tyrosine, phenylalanine, and/or tryptophan on a UAA test, as well as aluminum on HMT and/or UEE, you can consider using BH4. Run a CSA test and GI Test to rule out bacterial issues. |
| 3Hydroxyphenylacetic Acid4Hydroxyphenylacetic Acid | Increased 3 hydroxyphenylacetic acid and/or 4 hydroxyphenylacetic acid may be due to bacterial imbalances in your gut, or a need for BH4 so that tyrosine can be processed more fully. Lack of functional BH4 can be related to bacterial issues. Bacteria, in particular Staphylococci, sequester aluminum. Aluminum interferes with the activity of the DHPR enzyme needed to turn BH2 into BH4. Running a CSA test and GI Test helps to rule out bacterial issues. Also, use a UAA to check on tyrosine levels and the need for BH4. Consider addressing aluminum if HMT and UTM suggest elevated levels. Consider natural supports for BH4, including Royal Jelly if you have NO bee allergies, MTHFR A1298C Liver Support capsules, and BH4. Also consider support with gut herbs such as Naturomycin Spray, Naturomycin capsules, and grapefruit seed extract (GSE capsules or GSE liquid) along with probiotics. If aluminum is high, then use MetalAway, EDTA soap or EDTA soak. Run a CSA test and GI Test. |
| Dihydroxphenylpropionic Acid (DHPPA) | Dihydroxphenylpropionic acid (DHPPA) can be due to Clostridia, Pseudomonas, E.coli or Klebsiella. In order to specifically supplement based on particular organisms, run a CSA test & GI Test. General microbial support includes Naturomycin Spray plus Naturomycin capsules and grapefruit seed extract (GSE capsules or GSE liquid). You can consider BactiSolve if you have NO shellfish allergies to help address biofilm, along with EDTA soap /soak daily. Run a CSA test and GI Test to determine which microbes are the issue. If Clostridia is the greater concern based on testing or prior data, then consider using the full Clostridia support program. |
| Benzoic & Hippuric Acids | Benzoic and hippuric acids are breakdown products from phenylalanine. Excess tyrosine and tryptophan also feed into the pathway to hippuric acid. Phenylalanine, tyrosine, and tryptophan are all processed by BH4. If BH4 levels are not sufficient, or if excess aluminum is present, BH4 production may be impaired. This can drive up benzoic and hippuric acid levels. Check glycine levels on a UAA, because high glycine, in some cases secondary to SHMT +, can react with benzoic acid to form hippuric acid. High levels of support with TMG or betaine may increase both glycine and sarcosine, which can in turn increase hippuric acid levels and porphyrins. Consider natural supports for BH4, as well as addressing excess aluminum. Include MTHFR A1298C Liver Support capsules and MetalAway, as well as EDTA soap or EDTA soak. In addition, depending on your levels of phenylalanine, tyrosine, or tryptophan on a UAA, the aluminum on a HMT and UEE, or the values on a Neopterin / Biopterin Profile Urine Test, you can also consider BH4. |
| Arabinose & Citramalic Acid | Arabinose and citramalic acid are general indicators of excess yeast in your system. In order to determine if this is due to normal flora (Saccharomyces) or imbalanced flora, consider a CSA test and GI Test. If behavior or clinical presentation suggests that yeast or fungus are the issue, then consider support to address these issues. For adult females, the in-home Comprehensive Vaginosis Profile can also be run. To help address yeast imbalances, you can consider Candisol alternating with Lactoferrin, Mycology Support nucleotide blend, Naturomycin Spray, Naturomycin capsules, SHMT Spray and/or AHCY/SHMT compound and grapefruit seed extract (GSE capsules or GSE liquid). You may also consider BactiSolve if you do not have shellfish allergies. |
| Tartaric Acid | High tartaric acid can be due to yeast or fungal issues, or may result from a lack of B12. A HMT and UEE can help to determine if lack of B12 is the issue. You may also use a blood test for B12 levels. A high level of corpuscular hemoglobin (MCH) in your red blood cells is a marker for low B12. Be sure your lithium is in balance prior to adding extra B12, and determine the optimal form of B12 support based on your Nutrigenomic testing. If Nutrigenomic data is not available, use Hydroxy B12 and low dose Adenosyl B12. Consider a CSA test or GI Test to determine if the issue is yeast or fungal rather than a need for B12. If a CSA test and GI Test determine that yeast or fungus are the issues, then you can consider Candisol alternating with Lactoferrin, Mycology Support nucleotide blend, Naturomycin Spray, Naturomycin capsules, SHMT Spray, and/or AHCY/SHMT compound and grapefruit seed extract (GSE capsules or GSE liquid). You may also consider BactiSolve if you do not have shellfish allergies. If a lack of B12 is the issue, then consider low dose lithium support such as All in One and BeCalm Spray along with appropriate forms of B12. If Nutrigenomics are not known, then focus on Hydroxy B12 and Adenosyl B12, or Black Bear Spray or Black Bear Drink, which is a combination of hydroxy and adenosyl B12. |
| Lactic Acid & Pyruvic Acid | The MAP test has a helpful diagram that shows where lactic and pyruvic acids feed into the Krebs energy cycle. Pyruvic feeds into the Krebs energy cycle and is formed from carbohydrate via glucose, or can be from fats. Pyruvic acid is also formed from lactic acid with O2 and zinc. So, zinc will help you to cycle between lactic and pyruvic acids. The conversion of lactic or pyruvic acids into Krebs energy cycle substrates requires B vitamins. If lactic and/or pyruvic acids are building up, it would suggest that insufficient B vitamins are in place. Ultimate B Complex is a source of B complex that uses the most readily available forms of the B vitamins. Ultimate B Complex can be added, or add each of the B vitamins individually, such as Pantothenic Acid, Benfotiamine, Riboflavin-5-Phosphate and NADH or Niacinamide. Also, consider additional energetic support, since a buildup of lactic and pyruvic acids suggests that energy is not being generated appropriately from ingested food sources. Consider direct energy support with MitoForce, or add Carnitine, CoQ10, and/or Idebenone individually. Consider using Zinc, because when lactic acid gets too high, it can recycle to pyruvic acid with O2 and zinc. Some reports suggest the use of Yerba Mate to help with high levels of lactic acid due to exercise, so that lactic acid does not build up in your muscles and cause that painful, after-exercise soreness. Those who are ACAT+ may have particular issues converting food into energy. The individual components in the ACAT cap can be added one at time, or simply add ACAT/BHMT capsules. |
| Beta-Hydroxy-Butyric Acid (BHBA) | The buildup of beta-hydroxy-butyric acid (BHBA) is an indication that fats are not being processed ideally. It is a sign of possible ketosis. Often, higher levels of BHBA are seen in those who have H. pylori, or who do not have sufficient biotin and adenosyl B12 to process fats. Lack of pancreatic enzymes can also be a factor in high BHBA. Running a CSA test and GI Test to look at fatty acid processing may be useful. If there are other signs of low B12, such as high methylmalonic acid (MMA), low cobalt on a HMT and UEE, low lithium on a HMT, or low serum lithium, then supporting lithium and Adenosyl B12 may address high BHBA. If the issue is fat processing, then Biotin and digestive enzymes that are higher in pancreatin or bile salts may be a help. When high BHBA is a sign of possible ketosis, consider a UAA to check amino acid levels and a need for additional nutritional support. Consider using Biotin and Adenosyl B12 to help process fats. Also check to see if lithium support is needed. Consider using All in One and/or BeCalm Spray for low dose lithium support. Consider Special Digestive Enzymes as a source of enzymes high in pancreatin, and ACAT/BHMT capsules for low dose bile salt support. Also, consider MitoForce to help compensate for diminished energy components for the Krebs cycle. Certain diets may cause a greater tendency toward ketosis, such as the Specific Carbohydrate Diet or the Paleolithic Diet. A more balanced diet can be considered if these are factors in ketosis that do not resolve with supplement support. |
| Citric Acid | Citric acid, cis-aconitic acid, and isocitric acid are the first three metabolites in the Krebs Citric Acid energy production cycle, which operates in the mitochondria of your cells. Mitochondria are the structures within your cell that are your main source of energy. The terms citric acid, cis-aconitic acid, and isocitric acid can be used interchangeably with citrate, cis-aconate and isocitrate. They are just different forms of the same molecule. The same is true for any other organic acid. They have two names for two different forms of the substance, for example alpha ketoglutaric acid or alpha keto-glutarate, succinic acid or succinate, etc. These terms are used interchangeably throughout this chapter for the organic acids discussed. Aluminum has a particularly destructive effect on many steps of the Krebs Citric Acid Cycle. Aluminum interferes with the enzymes that convert citrate to isocitrate, so high levels of citrate and isocitrate may indicate that aluminum is high in your body. Additionally, lack of B12 can cause the Krebs energy cycle to run in the reverse direction leading to elevated citric acid. If a HMT and UEE indicate a need for more B12, then supplement the appropriate form of B12 for your genetics, after you are sure that your lithium is in balance. Lithium helps to transport B12 into your cells. If levels of lithium are low in hair, urine or serum, consider low dose lithium support. If citric acid is too low, consider increasing supports that help feed into the Krebs energy cycle, such as MitoForce and Ultimate B Complex. You can also consider supplements that supply citrate, such as Magnesium Citrate, Potassium Citrate, etc. Consider supporting with MitoForce or the individual components in MitoForce. Check HMT and UEE, and add B12 as needed once lithium is in balance. Use the low dose lithium support in All in One and/or BeCalm Spray when needed. Look for evidence of aluminum toxicity and consider MetalAway, EDTA soap or EDTA soak if aluminum is present. Consider natural supports for BH4, such as BH4 itself and MTHFR A1298C Liver Support capsules. You can also consider using Lactoferrin, Glutathione (GSH), and Vitamin K. High citric acid can be a sign of acidosis IF citric acid is high but cis-aconitic acid is NOT as high. Acidosis can occur from lack of bicarbonate due to decreased pancreatic enzymes, in which case consider Special Digestive Enzymes (SDE) which are high in pancreatin. If potassium is low on mineral tests, you can also consider low dose Potassium Bicarbonate. |
| Cis-Aconitic Acid | Aluminum interferes with the enzymes that convert citrate to isocitrate as well as the next step which converts isocitrate to alpha ketoglutarate (alpha KG), so high levels of cis-aconitate and isocitrate may indicate that your aluminum is high. Lack of B12 can cause the Krebs energy cycle to run in the reverse direction, potentially leading to elevated levels of citric acid, cis-aconitic acid, and isocitric acid. If a HMT and UEE indicate a need for more B12, then supplement B12 when you are sure that your lithium is in balance. Lithium helps to transport B12 into your cells. If levels of lithium are low in hair, urine or serum, use low dose lithium support. If citric acid is low, consider increasing supports that help feed into the Krebs energy cycle, such as MitoForce and Ultimate B Complex. Since iron and GSH play a role in the conversion of citric acid to cis-aconitic and isocitric acids, the use of supplements that help to move iron or support glutathione may also be a help when cis-aconitic acid levels are low. Consider supporting with MitoForce or the individual components in MitoForce. Check HMT and UEE, and add B12 as needed. Consider the low dose lithium support in All in One and/or BeCalm Spray when lithium is needed. Look for evidence of aluminum toxicity and consider MetalAway, EDTA soap or EDTA soak if it is present. Aluminum inhibits the DHPR enzyme that is necessary to convert BH2 into BH4. Consider natural supports for BH4, such as BH4 itself and MTHFR A1298C Liver Support capsules. You can also consider Lactoferrin, Glutathione (GSH), and Vitamin K. |
| Isocitric Acid | Aluminum interferes with the enzymes that convert citrate to isocitrate as well as the next step which converts isocitrate to alpha KG, so high levels of cis-aconitate and isocitrate may indicate that your aluminum is high. Lack of B12 can cause the Krebs energy cycle to run in the reverse direction, potentially leading to elevated levels of citric acid, cis-aconitic acid, and isocitric acid. If a HMT and UEE indicate a need for more B12, then supplement B12. Lithium helps to transport B12 into your cells. If levels of lithium are low in hair, urine or serum, consider low dose lithium support. Manganese, magnesium and vitamin B3 (ie. niacin, Niacinamide, or NADH) play a role in the conversion of isocitrate to alpha KG, so the use of these supplements may help if isocitric is high and alpha KG is lower. Conversely, if isocitrate levels are too low, consider increasing supports that help feed into the Krebs energy cycle, such as MitoForce and Ultimate B. Check HMT and UEE, and add B12 as needed. Consider the low dose lithium support in All in One and/or BeCalm Spray when needed. Look for evidence of aluminum toxicity and consider MetalAway, EDTA soap or EDTA soak. Consider natural supports for BH4, such as BH4 itself and MTHFR A1298C Liver Support capsules. You can also consider Ultimate B Complex, and Niacinamide or NADH. Check manganese and magnesium on a UEE and a HMT, and add as needed. Consider MitoForce or the individual components in MitoForce. |
| Alpha-Ketoglutaric Acid (alpha KG) | Aluminum can inhibit the reaction that converts glutamate to alpha KG, so low levels of alpha KG may be an indication of high aluminum. Check aluminum on a HMT and UEE, and support to address aluminum and BH4. If alpha KG is very low it may be due to high aluminum or a lack of B12. You may suspect that B12 is low especially if threonine, glycine and asparagine are high on a UAA. If the level of phosphate is low on a HMT or UEE, leucine may be increased. High leucine may also negatively impact alpha KG levels. Low alpha KG may cause hypoglycemia. Check leucine levels on a UAA. Determine if leucine is high in the absence of high isoleucine or high valine. If this is the case, consider using ATP and Riboflavin-5-Phosphate for phosphate support. If ammonia is very high on a UAA, and glutamate is also high, then much of the alpha KG may have been converted to glutamate. Work on high ammonia levels with CBS/NOS Kidney Support capsules. Check that sulfates are not too high, and check molybdenum levels. High levels of T4 thyroid hormone, thyroxine, inhibits the enzyme glutamate dehydrogenase, which then can increase glutamate levels and decrease alpha KG. Check a CSA test and GI Test, because imbalances in gut microbes can affect thyroid hormones. PABA, found in Ultimate B and Niacinamide can be considered for those who have concerns about thyroid autoimmunity. In addition, Coleus may be a help to support the thyroid. Look for evidence of aluminum toxicity and consider MetalAway, EDTA soap or EDTA soak if aluminum is present. Aluminum inhibits the DHPR enzyme that is necessary to convert BH2 into BH4, so consider natural supports for BH4, such as BH4 itself and MTHFR A1298C Liver Support capsules. If lack of B12 is an issue, consider All in One, BeCalm Spray, Hydroxy B12, Adenosyl B12, Black Bear Spray or Black Bear Drink. If alpha KG levels are too high, consider Ultimate B. If leucine is also high, consider ATP and Riboflavin-5-Phosphate. |
| Succinic Acid | Low succinic acid can be due to excess aluminum in your system. Look for other signs of aluminum excess, such as high aluminum on a HMT and UEE, imbalances in other Krebs cycle intermediates on the MAP, or a need for BH4 as evidenced by high phenylalanine, tyrosine, or tryptophan on a UAA. If these indicators suggest that aluminum and BH4 are issues, then consider MetalAway, EDTA soap, or EDTA soak, and BH4 supports, such as BH4 itself and MTHFR A1298C Liver Support capsules. In addition, succinate helps to limit the enzyme urocanase, which plays a role in increasing FIGLU and glutamate. So, low levels of succinate may be a factor in high FIGLU and high glutamate. If succinic acid is too low, consider Vitamin E succinate and Adenosyl B12. Low B2 (riboflavin) and B3 (niacin) generally lead to extremely high levels of succinic acid. If succinic acid is high, consider Riboflavin-5-Phosphate and MTHFR A1298C Liver Support capsules. In addition, consider NADH, Niacinamide or Ultimate B to support vitamin B3. Thallium can cause issues with riboflavin levels, so if thallium is present on the UTM or HMT, consider additional Riboflavin-5-Phosphate to help convert succinate to fumarate. High succinate may combine with excess glycine to increase porphyrins. Check glycine on a UAA, and use AHCY/SHMT compound if needed. |
| Fumaric Acid | Excess urea cycle function can generate high levels of fumarate, because fumaric acid is one of the urea cycle products. To see if excess urea cycle activity is causing high fumarate, look at a UAA to check arginine, ammonia, citrulline, and ornithine levels. High ammonia may drive your system to more urea cycle activity, so check ammonia on a UAA and support to address high ammonia if needed. Be sure the Krebs cycle is supported so that fumarate can be processed through the cycle. Specific nutrients such as Riboflavin-5-Phosphate, NADH , and/or MTHFR A1298C Liver Support capsules may be a help in processing fumarate. Support with MitoForce and sources of BH4 may help to shift the emphasis toward the Krebs energy cycle rather than on the urea cycle. A lack of B12 may cause the Krebs energy cycle to run in a reverse direction and cause increased levels of intermediates, including fumarate. Check markers for B12 levels, such as cobalt on a HMT and UEE, as well as methylmalonic acid (MMA) on a MAP test. Blood testing for B12 includes serum B12 levels and MCV. Be sure that lithium levels are in balance. In addition, check for and address high aluminum. Aluminum can interfere with the formation of BH4 that is needed for optimal urea cycle function. If BH4 appears to be low, consider supplementing BH4 or Royal Jelly if you have no bee allergies. For low levels of fumarate, consider Carnitine fumarate. |
| Malic acid | Low levels of malic acid have been implicated in fatigue. Check a MAP test for tartaric and citramalic acid levels. These acids can inhibit malic acid. Address those as needed if malic acid levels are low. When malic acid levels are low, consider support with Muscle Fatigue Support compound as well as eating apples. If levels of malic are high, consider Riboflavin-5-Phosphate, NADH, and/or MTHFR A1298C Liver Support capsules to help with the processing of malic acid. |
| Oxalic Acid |
A number of programs and tests focus on high oxalic acid, also called oxalate. In my program, the issue of high oxalate is integrated into my larger concern about overall biochemical balance. Aside from diet, there are a number of factors that may contribute to high oxalate levels. A determination if the trigger is, for example, high yeast or fungi, a lack of B12, or low ATP, is made through interpretation of testing. The reason for the high oxalate then guides your decisions as to how you address the problem. High oxalate may be due to yeast and fungal infestation. These factors can be investigated with a CSA test and GI Test, among others. Several chapters in this book contain suggestions for what to do when these issues are found.High oxalate can also be caused by low B12. Low B12 makes the Krebs cycle run in a reverse direction, which increases oxalate. Check cobalt levels on a UEE and HMT. Lithium transports B12 into your cells. Be sure that lithium is in balance with these two tests as well. The Krebs cycle is the energy/ATP generating portion of the mitochondria in your cells. Your level of B12 impacts enzymes in the Krebs cycle, and the levels of Krebs intermediates are affected. Adequate levels of B12 increase fumarate reductase, which then aids in processing oxalate and fumarate (Kurumada and Labbe Science Vol 151 page 1228).Conversely, lack of B12 leads to increases in citrate lyase and succinate dehydrogenase (Frenkel et al JBC Vol 251 page 2147). The net effect of these enzymatic changes is to increase oxalate and fumarate levels. While fumarate is generally converted to malate, it may happen that when fumarate levels are high enough, some of it is converted to tartarate. Feedback inhibition by high oxalate in addition to high fumarate may control the flow into malate, such that fumarate and oxalate are converted to tartarate. The pathway that leads to formation of tartarate from oxalate has been defined (Nakamura and Ogata, JBC Vol 248 page528 and Shreeve and Meuter JBC Vol 239 page 729), as has as the path from fumarate to tartarate (Kuni and Hernandez JBC page 201 and Finkle JBC page 349).Conditions of B12 deficiency, coming either as a result of mutations in the methylation cycle, and/or by high level depletion of B12 through endurance training or sports, can lead to increased levels of tartarate, fumarate, and oxalate. High levels of tartarate in the absence of high arabinose, or high levels of fumarate, should lead you to consider supplementing with multiple forms and routes of B12. This includes chewable hydroxyl, adenosyl, and methyl B12. The relative amounts depend on your Nutrigenomics. If you have high oxalate levels, you should consider increasing your B12 support for an additional reason. Relative B12 deficiency increases the conversion of citrate to oxalate via citrate lyase. Consider Lactoferrin, Vitamin K, Pantothenic Acid, Riboflavin-5-Phosphate, Curcumin, Benfotiamine, and GSH to increase the flow from pyruvate through citrate and onto isocitrate as another way to decrease high oxalate. The use of MitoForce may also support this conversion. High leucine in the absence of high valine or isoleucine can occur secondary to low phosphate. This can also cause increases in oxalate, so check to determine if leucine is high on a UAA. If so, consider ATP and Riboflavin-5-Phosphate to support phosphate. High oxalate may also be due to excess glycine secondary to SHMT + or excess iron. Glycine can be checked on a UAA, and iron levels are on a UEE and HMT. As discussed in the UAA chapter, high glycine can be addressed with supports for SHMT. If threonine is high on a UAA test, this may be an indication of high oxalic acid. High levels of oxalates may increase ACE activity. The use of anxiety support and progesterone may be helpful. (Umekawa et al J. Am Soc Nephrol Vol 15, 2004). High levels of citrate or high levels of the intermediates that precede acetyl CoA on the MAP diagram, i.e., pyruvate, lactate, etc., may be an indirect indication of high oxalate, as the cycle is not incorporating at 11:00 (oxalate) well enough to be moving around to 1:00 (citrate) properly. Also, a build up at 1:00 (citrate) may be causing a backup in the cycle, which may be an indirect indication of high oxalate. Consider MitoForce or Lactoferrin, Vitamin K, Riboflavin-5-Phosphate, Pantothenic Acid, and Benfotiamine to get the portion of the cycle from 11:00 to 1:00 moving. Those who are ACAT + may also have problems converting nutrients from food into the Krebs energy cycle, and the use of ACAT/BHMT capsules may be a help in this regard. Research articles illustrate a relationship between B12 and ATP which seems to present a catch 22. ATP, the fuel generated by your body to drive its biochemical reactions, is created by your Krebs energy cycle. The Krebs cycle needs B12 in order to function optimally. If your Krebs cycle is not functioning optimally, ATP production is reduced. Yet, ATP is needed to transport B12 into your cells. However, lithium also plays a role in B12 transport, so lithium levels should be checked and supported as needed. MitoForce or ATP, NADH, Vitamin E succinate, and Malic Acid also play a role in B12 transport and may be supplemented as needed. High levels of sulfur in your system can have a negative impact on the regeneration of ATP and NADH. This may be a particular issue for those who are SUOX + – or CBS ++. MitoForce or ATP, NADH, Vitamin E succinate, and Malic Acid help to regenerate these important intermediates also. The supplements suggested for consideration to reduce high oxalate depend upon its cause. If low B12 is the issue, consider a source of low dose lithium, such as All in One and/or BeCalm Spray, in addition to B12 itself. If high glycine and/or high iron are the issues, consider SHMT support. If leucine alone is elevated on a UAA, without concurrent increases in isoleucine and valine, then consider ATP and Riboflavin-5-Phosphate . Aluminum and thallium can impair the function of the Krebs cycle, so address thallium and aluminum if they are found to be elevated on HMT, UTM or FMT. |
| Beta-Hydroxy-Beta-Methylglutaric Acid (HMG) | Similar to BHBA, high levels of HMG suggest problems processing nutrients to convert them into energy via the Krebs cycle. Studies suggest that Carnitine may be a particular help. To help convert nutrients into energy, consider MitoForce and additional Carnitine. If you are not using MitoForce, then individually add the other ingredients in the MitoForce compounded supplement, such as CoQ10, Benfotiamine, Riboflavin-5-Phosphate, Pantothenic Acid, Policosanol, and Cholacol or ACAT/BHMT capsules to help process fats.Also, rule out excessively high leucine on a UAA. If high leucine is present in the absence of elevated valine or isoleucine, then consider Riboflavin-5-Phosphate and ATP to support phosphate levels. |
| Adipic Acid | High adipic acid suggests fat processing problems. Biotin, low dose Adenosyl B12, and Special Digestive Enzymes (SDE) may be a help. Consider a CSA test and GI Test to look at short chain fatty acids. To help process fats, consider Carnitine and SDE. Also, consider MitoForce or add the other ingredients in the MitoForce compounded supplement, such as CoQ10, Benfotiamine, Riboflavin-5-Phosphate . Pantothenic Acid, Policosanol, and Cholacol or ACAT/BHMT capsules to help process fats. |
| Suberic Acid | High suberic acid suggests a strong need for carnitine. High suberic acid is often seen with H. pylori. This organism may deplete carnitine. Consider ruling out H. pylori with a breath test, or running a CSA test and GI Test to look at other possible markers for H. pylori, including gut pH. Carnitine support is the key approach to high suberic acid. Also, consider MitoForce or add the other ingredients in the MitoForce compounded supplement, such as CoQ10, Benfotiamine, Riboflavin-5-Phosphate , Pantothenic Acid, Policosanol, and Cholacol or ACAT/BHMT capsules to help process fats. If you are concerned that H. pylori may be the cause of your high suberic acid because of other markers as well as clinical presentation, then you and your doctor can consider the more complete H. pylori protocol used in this program. A more mainstream approach to H. pylori is a triple prescription therapy, including minocycline, augmentin, and proton pump inhibitors. |
| Vanilmandelic Acid (VMA) | VMA is a breakdown product from both epinephrine and norepinephrine. This MAP test also measures MHPG, which is a reflection of primarily the breakdown of norepinephrine. So, comparing VMA to MHPG gives you a sense of whether there is excessive breakdown of both, or only increased breakdown of norepinephrine. It has been suggested that higher norepinephrine activity relative to epinephrine is a factor in ADD/ADHD. This is a reason to pay attention to the ratio of VMA to MHPG. If the values are very elevated, consider a Neurotransmitter Test (NT test) to look directly at epinephrine and norepinephrine levels in addition to their breakdown products. If MHPG levels are higher than VMA, consider using Vitamin C, because ascorbic acid may shift the balance to higher levels of epinephrine relative to norepinephrine. Also, consider Phosphatidyl Serine Complex (PS/PE/PC) and low dose Attention Support nucleotide blend. SAM-e may also be helpful, depending on your Nutrigenomics. For very high levels of VMA, also consider low dose Mood D nucleotide blend. Recent studies suggest that Yohimbe may be a help in shifting to higher levels of epinephrine relative to norepinephrine. Yohimbe is also reported to help with fat digestion and healthy insulin levels. However, Yohimbe has also been suggested to help with erectile dysfunction; for this reason, it should be used with caution in children and teens. When your main concern is attention, focus, depression, ADD, ADHD or OCD, then consider looking at neurotransmitters in several ways. In addition to looking at the breakdown products on a MAP test, also consider a Neurotransmitter Test (NT Test) to get the level of the NT, as well as a UAA to assess the level of starting material to make NT and, if needed, a Neopterin / Biopterin Profile Urine Test. In this way, you look at breakdown on a MAP, the levels of neurotransmitters on a NT test, and the level of the starting material for producing neurotransmitters on a UAA and biopterin test. |
| Homovanillic Acid (HVA) | HVA is the breakdown product of dopamine. If your values are very low, then some additional support for dopamine production may be a help. Alternately, support for the process that breaks down dopamine via Mao B may be needed. Additional testing can help to differentiate between these options. Consider a NT test to be sure that dopamine is in the normal range. Use a UAA to see if there is sufficient tyrosine to produce dopamine, and if there is evidence of sufficient BH4 to convert tyrosine into dopamine. If dopamine is high on a neurotransmitter test, yet the HVA is low on a MAP, copper levels may be too low. Dopamine is processed by the enzyme MAO B. This enzyme requires copper to function. In addition, MAO B may be inhibited due to high levels of hydrogen sulfide, which can decrease MAO activity. If levels of HVA are very low, run a UAA to look at tyrosine levels to be sure there is sufficient material for the body to produce dopamine. In addition, MAO B may be inhibited due to high levels of hydrogen sulfide, which can decrease MAO activity. In this case, looking at taurine levels and certain transulfuration markers, such as cysteine, cystathionine, cystine, and glutathione on the UAA may also be helpful. Also consider sulfur levels on a HMT and UEE to determine if this may be a cause of low HVA. Licorice may inhibit MAO enzymes, so limit the use of licorice if levels of HVA are very low. If low HVA is ALSO associated with low dopamine on an NT test, then ascertain that there is sufficient tyrosine and BH4 to make dopamine. You may need to consider direct, low dose, natural supports for dopamine. These include low dose Ginkgo Biloba, Mucuna Pruriens, Mycoceutics, low dose Mood D nucleotide blend, and low dose Mood Focus nucleotide blend, depending on your nutrigenomics. As always, work with and defer to your own doctor, especially when addressing imbalances in neurotransmitters. Conversely, if values of HVA are high, run a HMT and UEE to check copper levels. Be sure that copper is not higher than zinc. The use of Molybdenum, Manganese and low dose EDTA may help if copper levels are high. This may help to get copper into better balance, and to slow down excessive dopamine breakdown, which would lead to high HVA levels. When your main concern is attention, focus, depression, ADD, ADHD or OCD, then consider looking at neurotransmitters in a range of ways, not just the breakdown products on a MAP test. Also consider a NT test, as well as a UAA, and, if needed, a Neopterin / Biopterin Profile Urine Test. In this way, you look at breakdown on a MAP, levels of neurotransmitters on a NT test, and starting material for producing neurotransmitters on a UAA and biopterin test. |
| 5-OH-Indoleacetic Acid (5-HIAA) | 5 HIAA is a breakdown product of serotonin. Serotonin is broken down by the enzyme MAO A. This enzyme requires copper to function. If 5 HIAA is high, run a HMT and UEE to check copper levels. Be sure that copper is not higher than zinc. The use of Molybdenum, Manganese and low dose EDTA may help if copper levels are high. If levels of 5HIAA are very low, yet serotonin is high on a NT test, then MAO A may be inhibited due to high levels of hydrogen sulfide, which can decrease MAO activity. In this case, run a UAA to look at taurine levels and certain transulfuration markers, such as cysteine, cystathionine, cystine, and glutathione. Look at sulfur on a HMT and UEE to determine if this may be a cause of low 5HIAA.Also, if serotonin is high on a NT test, and 5HIAA is low, be sure that copper levels are not too low. Licorice also may inhibit MAO enzymes, so limit the use of licorice if levels of 5HIAA are very low. Low levels of serotonin have been associated with OCD and perseverative behavior, as well as depression. I suggest that you look at neurotransmitters in a range of ways, not just the breakdown products on a MAP test. So consider a NT test, as well as a UAA, and, if needed, a Neopterin / Biopterin Profile Urine Test. In this way, you look at breakdown on a MAP, levels of neurotransmitters on a NT test, and starting material for producing neurotransmitters on a UAA and biopterin test.For high levels of 5HIAA, consider low dose Mood S nucleotide blend and low dose SeroMood. Be sure that copper levels are not high, and that molybdenum and manganese are not low. Check tryptophan on a UAA and serotonin on a NT test. Check for signs that BH4 needs support or that excess aluminum is impacting BH4.Serotonin levels can be impacted by bacterial issues. Especially if the bacterial markers on a MAP are elevated, you should do a CSA test and GI Test. Also, in the case of high bacterial markers, consider support for vitamin B3, niacin, with Ultimate B and MTHFR A1298C Liver Support capsules. |
| 3-Methyl-4-OH-phenylglycol (MHPG) | MHPG is the breakdown product from norepinephrine, but it may also be produced from epinephrine to a lesser extent. Still, comparing VMA to MHPG gives you a sense of whether there is excessive breakdown of both, or only increased breakdown of norepinephrine. When norepinephrine is too high relative to epinephrine, it may cause decreased ability to focus and attend. High levels of norepinephrine may decrease BH4, so consider other testing to be sure that sufficient BH4 is available. When your main concern is attention, focus, depression, ADD, ADHD or OCD, then consider looking at neurotransmitters in a range of ways, not just the breakdown products on a MAP test. So, consider a NT test, as well as a UAA, and, if needed, a Neopterin / Biopterin Profile Urine Test. In this way, you look at breakdown on a MAP, levels of neurotransmitters on a NT test, and starting material for producing neurotransmitters on a UAA and biopterin test. Supplements that may help with attention include low dose Attention Support nucleotide blend, NADH, MTHFR A1298C Liver Support capsules, BH4, Royal Jelly if you have NO bee allergies, DMG, SAM-e, Phosphatidyl Serine Complex (PS/PE/PC) and Zinc. If MHPG levels are higher than VMA, consider using Vitamin C. Ascorbic acid may shift the balance to higher levels of epinephrine relative to norepinephrine. Recent studies suggest that Yohimbe may be a help in shifting to higher levels of epinephrine relative to norepinephrine. Yohimbe is also reported to help with fat digestion and with healthy insulin levels. However, Yohimbe has also been suggested to help with erectile dysfunction. For this reason, it should be used with caution in children or teens. |
| Kynurenic Acid | Kynurenic acid is a breakdown product of tryptophan. Use a UAA to check that tryptophan levels are in balance, and neopterin/biopterin testing to determine if sufficient BH4 is present to convert tryptophan into serotonin. Also, use a NT test to check NT levels. Kynurenic acid is a calming compound, but it will convert to quinolinic acid in the presence of B6. This is a concern because quinolinic acid is an excitotoxin. High kynurenic and/or quinolinic acids may be due to bacterial issues. Use a CSA test and a GI Test to rule out excess non-ideal microbes. Support for high kynurenic acid includes MTHFR A1298C Liver Support capsules to help natural levels of NADH, Niacinamide and healthy BH4. Consider adding BH4 depending on the UAA, and a Neopterin / Biopterin Profile Urine Test if it appears that high kynurenic acid is due to lack of BH4 and decreased serotonin. If both kynurenic and quinolinic acids are high, then limit B6 and Pyridoxal-5-phosphate (P5P) to attempt to shift the balance to kynurenic rather than quinolinic acid. If bacterial issues are suspected, you can consider Naturomycin Spray, Naturomycin capsules, grapefruit seed extract (GSE capsules or GSE liquid) and BactiSolve if you have NO shellfish allergies. |
| Quinolinic Acid | Kynurenic acid, which is derived from the processing of tryptophan, is converted to quinolinic acid in the presence of B6 or P5P. While kynurenic is calming, quinolinic is an excitotoxin that can over stimulate nerves. Excitotoxins can cause seizure activity, problems sleeping, heart palpitations, nervous twitches, among other symptoms. Consider GABA Balance capsules, BeCalm Spray, and Nerve Calm nucleotide blend. Consider a CSA test and GI Test to check for bacterial issues that may be involved with breaking down tryptophan, and to look at which specific microbes may need to be addressed. For high levels of quinolinic acid from bacterial breakdown, consider BactiSolve if you have NO shellfish allergies, Naturomycin Spray, Naturomycin capsules, and grapefruit seed extract (GSE capsules or GSE liquid). Limit B6 and P5P. |
| a-Ketoadipic Acid (AKAA) | As with any of the keto acids, ketosis may be an issue when high AKAA is present. Ketosis can be a factor in lack of growth or poor weight gain. If you are using a diet that can increase ketosis such as the Specific Carbohydrate Diet or Paleolithic Diet, be aware that they may be a factor in high keto acids. The use of Biotin and low dose Adenosyl B12 may be a help for ketosis. AKAA is formed from tryptophan and lysine, so be sure that excess lysine is not being added to your diet. See that there is sufficient BH4 to process tryptophan into serotonin. You may also check serotonin levels on a NT test and tryptophan and lysine levels on a UAA. To support healthy levels of BH4, consider supplementing BH4 itself if other tests indicate a need. You can also use MTHFR A1298C Liver Support capsules. In addition, use Ultimate B to help support B vitamin cofactors. AKAA is a precursor to glutaric acid, so also consider supplementing with Carnitine, as Carnitine is reported to help mitigate the effects of glutaric acid. Run a CSA test and GI Test to rule out bacterial production of AKAA. If bacterial issues are a concern, use gut herbs, including Naturomycin Spray, Naturomycin capsules, and grapefruit seed extract (GSE capsules or GSE liquid). Rule out H. pylori if other markers or clinical presentations for that bacteria are present, such as history of acid reflux, etc. |
| a-Ketoisovaleric Acid (AKIV) | As with any of the keto acids, ketosis may be an issue when high AKAA is present. Ketosis can be a factor in lack of growth or poor weight gain. If you are using a diet that can increase ketosis such as the Specific Carbohydrate Diet or Paleolithic Diet, be aware that they may be a factor in high keto acids. AKIV is specifically due to breakdown of valine. Excess levels of the branched chain amino acids (BCAA) of valine, leucine and isoleucine can cause a maple syrup smell to your urine. Decreasing the use of BCAA can help.The use of Biotin and low dose Adenosyl B12 may be a help for ketosis. Ultimate B can be used to help support B vitamin cofactors for the processing of fats. Also, consider using MitoForce and additional Carnitine. This is important, because high levels of BCAA and their respective ketoacids have been implicated in depletion of mitochondrial energy, which has significant negative effects on your system. Consider support with SDE to help with fat digestion, and ACAT/BHMT capsules if needed to help get fatty acids into a normal, healthy range.Rule out H. pylori. With any case of suspected ketosis, run a CSA test and GI Test to check on the processing of fats. Check a UAA to see that nutrients are in fact being absorbed. You can also run an Intestinal Permeability test. The Celiac test can also be run if desired. |
| a-Ketoisocaproic Acid (AKIC) | As with any of the keto acids, ketosis may be an issue when high AKAA is present. Ketosis can be a factor in lack of growth or poor weight gain. If you are using a diet that can increase ketosis such as the Specific Carbohydrate Diet or Paleolithic Diet, be aware that they may be a factor in high keto acids. AKIC is specifically due to breakdown of leucine. Excess levels of the branched chain amino acids (BCAA) of valine, leucine and isoleucine can cause a maple syrup smell to your urine. A body odor that smells like “sweaty feet” may be an indication of leucine breakdown issues. Decreasing the use of BCAA can help.The use of Biotin and low dose Adenosyl B12 may be a help for ketosis. Support with Ultimate B to supplement B vitamin cofactors. Also, consider using MitoForce and additional Carnitine. This is important, as high levels of BCAA and their respective ketoacids have been implicated in depletion of mitochondrial energy that has significant negative effects on your system. Support with SDE to help fat digestion and use ACAT/BHMT capsules if needed to get fatty acids into a normal, healthy range. If only AKIC is elevated without an elevation in AKIV or AKBM, then consider that low phosphate may be increasing leucine levels. Check phosphate levels on a HMT and UEE and support with ATP and Riboflavin-5-Phosphate if the levels of phosphate are low. Rule out H. pylori as with any case of suspected ketosis, and run a CSA test and GI Test to check on the processing of fats. Check a UAA to see that nutrients are being absorbed. Conversely, low levels of AKIC may be a factor in absence seizures, along with low levels of leucine in particular and BCAA in general. If levels of AKIC are very low, along with low levels of BCAA on a UAA, then consider BCAA support and AminoAssist. Be sure that no maple syrup smell comes to your urine due to too much support. This is important, as high levels of BCAA and their respective ketoacids are an issue as described above. However, extremely low levels are a risk factor for other health conditions. |
| a-Keto-b-Methylvaleric Acid (AKBM) | As with any of the keto acids, ketosis may be an issue when high AKAA is present. Ketosis can be a factor in lack of growth or poor weight gain. If you are using a diet that can increase ketosis such as the Specific Carbohydrate Diet or Paleolithic Diet, be aware that they may be a factor in high keto acids. AKBM is specifically due to breakdown of isoleucine. Excess levels of the branched chain amino acids (BCAA) of valine, leucine and isoleucine can cause a maple syrup smell to your urine. Decreasing the use of BCAA can help. The use of Biotin and low dose Adenosyl B12 may be a help for ketosis. In addition, Ultimate B may help to support B vitamin cofactors. Also, consider MitoForce and additional Carnitine. This is important, as high levels of BCAA and their respective ketoacids have been implicated in depletion of mitochondrial energy that has significant negative effects on your system. Support with SDE to help with fat digestion and use ACAT/BHMT capsules if needed to help get fatty acids into a normal, healthy range. Rule out H. pylori as with any case of suspected ketosis, and run a CSA test and GI Test to check on the processing of fats. Check a UAA to be sure that nutrients are being absorbed. |
| Formiminoglutamic Acid (FIGIU) |
High FIGLU suggests that adequate folate is not in place. All in One supplies low doses of folic acid, folinic acid, and 5 methyl THF. There are two key reasons to support with low doses of folate/folic acid, in addition to the use of specific types of folate such as 5 methyl THF that help to bypass mutations like MTHFR C677T. First, since 1959 it has been known that “folic acid deficiency results in inability to degrade formiminoglutamic acid (FIGLU) to glutamic acid, so that FIGLU accumulates in excessive amounts and is excreted in the urine”. (Luhby, Am J Clin Nutr). FILGU levels are measured on this MAP test, and high levels suggest a need to use low dose folate/folic acid support. The second reason to look at low dose folic acid/folate is the pathway that involves MTHFS. A low dose form of plain folate or folic acid is supplemented in part to address possible MTHFS mutations, especially since they are not generally identified on most nutrigenomic tests. MTHFS is another enzyme in the methylation pathway. It functions at 11:00 in the folate cycle, between 5 formyl THF (folinic) on the way to produce tetrahydrofolate at 12:00. MTHFS functions to address SHMT and the formation of the purines guanine and adenine for DNA and RNA formation. If there is a mutation that impacts the ability of MTHFS to function, it can increase folinic acid to high levels and limit the synthesis of purines, as well as decrease the THF level. In this program, my policy is to use only low dose folinic acid, to add nucleotides to support DNA and RNA production, and to use low dose folic acid along with probiotics as a secondary way to make THF. In this way, I bypass the impact of any possible MTHFS mutation, even if I do not have nutrigenomic data regarding this gene. This again highlights why I want to think about all aspects of the pathway when adding support. I choose to add only low dose folinic acid to help keep SHMT in balance without allowing the levels of folinic to climb, which might happen if you are adding high dose folinic and have a MTHFS mutation. I add nucleotides to supply purines and pyrimidines in case the pathway for their formation is not fully functional. I add low dose folic acid to have a secondary route for making THF that consumes excess glutamate in doing this. The rationale behind also adding low dose 5 methyl THF is that the way to bypass an MTHFR C677T mutation is with 5 methyl THF. If you look at the biochemical diagrams you can see this. No amount of folinic, folate, or folic acid is going to bypass a MTHFR C677T mutation. So, the whole conversation about folic acid or folate is actually misplaced, as the real issue is 5 methyl THF. There is some sort of misconception out there that folate will bypass MTHFR. To be clear, 5 methyl THF is the only way to bypass MTHFR C677T. I have it in low dose form in both All in One as well as Methylmate B. If you are C677T ++, using high dose 5 methyl THF can trigger more detox than you can handle, especially if you are an adult. This is why All in One uses low dose 5 methyl THF, and my stand alone source of 5 methyl THF, Methylmate B, is a liquid, so you have exquisite control over increasing or decreasing its dose. MOST of the folate that is used for this program is 5 methyl THF, with some low dose folinic acid. Folinic is useful for those who are SHMT + or have iron levels that may increase SHMT activity. Some low dose folic acid/folate is helpful for other aspects of the pathway, and that is why some very, very low dose folic acid is included in the formulation.To summarize, I do feel that some low dose folinic acid is needed to help to control SHMT, which is why All in One also has some low dose folinic. I do not like high dose folinic as those with MTHFS mutations can have a problem with it. Finally, for adequate processing of FIGLU, I want some low dose folate/folic acid in your system. Because the various forms of folate compete with each other for transport into your cells, the ratio in the All in One is mostly 5 methylTHF, with a lesser amount of folinic, and finally the least amount of folic acid.Now I am going to be very specific with regard to why I use low dose folic acid rather than folate. Folate is basically a chain of glutamates. The difference between folic acid and folate is the stability and the length of their glutamate chains. So, if you are MTHFR C677T++ and you take high dose folate, you potentially have a chain of unused glutamate molecules left in your system. You cannot process it efficiently to 5 methyl THF because of your SNPs. You run the risk of folate breaking down to release glutamate into your system. STEP 1 of this program is focused on glutamate/GABA balance. I have made significant progress for some individuals merely by getting their glutamate and GABA into balance. Thus, I am not choosing to add high doses of a form of folate that could break down into glutamate, especially in the population I work with. One of the main differences between folic acid and folate is that folic acid has a shorter glutamate chain than folate. Folic acid is also more stable, so it is less likely to break down into glutamate. I am using only a tiny bit of folic acid, to allow FIGLU to convert to glutamic acid. I am not using high dose folic acid, as that is not going to bypass MTHFR in any event. I understand there are other programs out there that use higher doses of plain folate. Perhaps those programs are less concerned with the glutamate issue. I have specific reasons for the choices I make in terms of supplements and the forms that I use. Natural folate has more glutamate residues and can break down more easily to release those glutamate molecules into your system, so I prefer to use a VERY low dose of folic acid. There are only approximately 15 micrograms of folic acid in All in One and about 25 micrograms in Ultimate B. This program uses some very, very low dose folic acid for the reactions that need it, but the focus is more heavily on the use of 5 methyl THF and low dose folinic acid. The use of LOW dose folic acid is a choice, to limit the risk of increased glutamate in your system. The RDA for folate/folic acid is 300 micrograms for a child that is 1 year old, up to 1,000 micrograms daily for an individual 19 years of age or older. Thus the 15 to 40 micrograms used for this program is not an issue, especially since the body does need some folate/folic acid aside from the need for 5 methyl THF and folinic. To put this in an easily understandable perspective, a bowl of cheerios has 400 micrograms of folic acid, as compared to the 15 to 40 micrograms used in this program. In addition to making rational choices in terms of folic acid versus folate, and only using low dose folinic out of consideration for possible MTHFS mutations, I am already taking into account the need to balance the production of purines, thymidine levels, controlling SHMT, and producing methionine from homocysteine with the supplementation I have in place for the methylation cycle. To reiterate the approach: (1) get the BHMT pathway moving with Phosphatidyl Serine Complex (PS/PE/PC) plus DHA, SAM-e if tolerated, All in One, Ultimate B, and low dose methylation RNA; (2) add some low dose lithium support with BeCalm Spray, and run a HMT to be sure you have checked lithium to see if you need low dose Lithium Orotate. If aggression is an issue, pay close attention to potassium and rubidium on your HMT. If your lithium is very low, run a HMT every 3 to 4 months to keep an eye on levels; (3) once lithium is in balance, you can add extra B12; (4) add Methylmate A and Methylmate B to be sure you have the cycle fully supported; (5) if you have SHMT + status or high iron on HMT and UEE, use SHMT support along with step 1 and 2 above; (6) be sure you have probiotics in place, focusing on Lactobacillus and Bifidobacter; (7) run a HMT to check lithium every few months once you have extra B12 in place. High levels of the enzyme urocanase will also increase FIGLU. Urocanase is produced by certain bacteria, including Pseudomonas, so consider a CSA test and GI Test when high FIGLU is noted on a MAP. Urocanase is limited by succinate. Be sure that succinate levels on a MAP test are in balance, because a lack of succinate combined with bacterial increases in urocanase can be factors in high FIGLU in addition to a need for folate. In terms of support for high levels of FIGLU, the use of All in One supplies specialized forms of folate. Also, once it is clear that lithium is in balance on a HMT, consider low dose Methylmate A and Methylmate B for comprehensive methylation support. Use Vitamin E succinate if succinate levels are low. Also, consider a CSA test and GI Test to rule out Pseudomonas. Consider the use of gut herbs including Naturomycin Spray, Naturomycin capsules, and grapefruit seed extract (GSE capsules or GSE liquid) when necessary. |
| Glutaric Acid | Glutaric acid is a breakdown product of lysine and/or tryptophan, so limit lysine support. Run a UAA to be sure that tryptophan is being converted properly to serotonin, that adequate BH4 is present, as well as checking serotonin levels on a NT test. Glutaric acid is also produced by bacteria, so consider a CSA test and GI Test. Carnitine is reported to help mitigate the effects of glutaric acid, so consider extra Carnitine support. If bacterial issues are a concern, then use grapefruit seed extract (GSE capsules or GSE liquid), Naturomycin Spray, and Naturomycin capsules. |
| Isovalerylglycine | Isovalerylglycine is a breakdown product of leucine. As with AKIC, it may be a sign of ketosis, so consider using Biotin and Adenosyl B12. Limit leucine and BCAA, increase Carnitine, CoQ10 spray, and low dose GABA Calm. Also, consider Ultimate B and MitoForce. Add carbohydrates from well thought out sources if ketosis is present. A body odor that smells like “sweaty feet” may be an indication of leucine breakdown issues. If only isovalerylglycine and AKIC are elevated without increases in AKIV or AKBM, then low phosphate may be the issue. You can support with Riboflavin-5-Phosphate, ATP and MitoForce. Rule out H. pylori with any case of suspected ketosis. Run a CSA test and GI Test to check on the processing of fats. To help with fat digestion, consider SDE and ACAT/BHMT capsules if needed. Run a UAA to be sure that nutrients are being absorbed. Also, check glycine levels on a UAA and iron on a HMT and UEE. If glycine and/or iron are elevated, consider AHCY/SHMT compound and SHMT Spray for support.In cases of very high isovalerylglycine levels, seizures may be present. In these cases, consider support for glutamate and GABA balance, such as GABA Balance capsules, Nerve Calm nucleotide blend, and BeCalm Spray. |
| Methylmalonic Acid (MMA) | MMA is most often considered to be a sign of low B12, which it is. However, it is also related to the breakdown of the branched chain amino acids (BCAA) of leucine, isoleucine, and valine. If high methylmalonic acid is seen on a MAP and high leucine on a UAA, consider using low dose Adenosyl B12 and Biotin. High levels of MMA may be associated with a maple syrup smell from your urine. MMA may enhance the impact of excess glutamate, so consider supports to balance glutamate, such as GABA Balance capsules, Nerve Calm nucleotide blend, and BeCalm Spray. Excess MMA can react with high glycine to increase porphyrins. Check glycine on a UAA. Use SHMT Spray and AHCY/SHMT compound as needed to help keep glycine in balance. When MMA is high, limit BCAA support, and use Adenosyl B12 and Biotin to help with its processing. |
| Xanthurenic Acid | Xanthurenic acid is related to the processing of tryptophan. Use a UAA to check that tryptophan levels are in balance, and consider testing to determine if sufficient BH4 is present to help convert tryptophan to serotonin. Also, use a NT test to check NT levels. Compare the level of xanthurenic acid on a MAP test to serotonin on a NT test and tryptophan on a UAA, as this may help indicate if BH4 support is needed.Xanthurenic acid also suggests a need for more B vitamins, including B6, so consider using Ultimate B. Xanthurenic acid may increase the impact of glutamate, so consider supplements to calm glutamate, including GABA Balance capsules, Nerve Calm nucleotide blend, and BeCalm Spray. Consider support for BH4 if the composite of tests suggest a need for BH4 support. These include MTHFR A1298C Liver Support capsules, BH4, and Royal Jelly if you do not have any bee allergies. |
| 3-Hydroxyproprionic Acid (3HPA) | 3HPA is a precursor to MMA. Excess MMA is due to the breakdown of branched chain amino acids (BCAA) of leucine, isoleucine and valine. Limit BCAA support. Also, consider Adenosyl B12 and Biotin to help with processing them. See additional suggestions listed under MMA above. High levels of MMA may be associated with a maple syrup smell from the urine. MMA may enhance the impact of excess glutamate, so consider supports to balance glutamate. These include GABA Balance capsules, Nerve Calm nucleotide blend, and BeCalm Spray. |
| 3-Hydroxyisovaleric Acid | Ketosis of any type can cause a non specific elevation in hydroxyisovaleric acid. With high hydroxyisovaleric acid, consider support with Biotin and Adenosyl B12 to help with ketosis, and run a CSA test and GI Test to check on the processing of fats. Rule out H. pylori as with any case of suspected ketosis. Use a UAA to be sure that nutrients are being absorbed. Biotin, Adenosyl B12, MitoForce, and extra Carnitine can be used for ketosis. Consider BeCalm Spray, GABA Balance capsules and Nerve Calm nucleotide blend for glutamate issues related to ketosis. Consider SDE to help with fat digestion and ACAT/BHMT capsules if needed. If you are using a diet that can increase ketosis such as the Specific Carbohydrate Diet or Paleolithic Diet, be aware that they may contribute to high keto acids. |
| α-Ketophenylacetic Acid (from styrene) &α-Hydroxyisobutyric Acid (from MTBE) | When high levels of these two toxic breakdown products are found, the function of support systems such as the liver and kidneys may be impaired by excess toxin exposure. B12 may play a role in processing these compounds, so use low dose B12, and be sure lithium is in balance to help with B12 transport into the cells. Check lithium on a HMT and UEE prior to adding more B12 than the low levels found in All in One. Consider Liver Support nucleotide blend, and MTHFR A1298C Liver Support capsules. Consider GSH and Quercetin to help with possible DNA damage, along with the use of Ultifend, SHMT Spray and AHCY/SHMT compound supply nucleotides. Also, consider Ora-Kidney and Kidney Support nucleotide blend. |
| Orotic Acid | Orotic acid lies along the biochemical route for making DNA building blocks. When levels of orotic acid are high, use ATP to convert the orotic that has built up into pyrimidines. Also, use SHMT Spray, AHCY/SHMT compound, and All in One to supply nucleotides to your system. Excess orotic acid may be a sign of increased ammonia, so consider a UAA and address excess ammonia if needed. Consider CBS/NOS Kidney Support capsules to help ammonia detox.Be sure that methylation support is in place so that you can produce thymidine from uridine, which is the next step after orotic acid. Basic methylation support includes All in One, Phosphatidyl Serine Complex (PS/PE/PC), DHA and Methylation Support nucleotide blend. Once lithium is shown to be in balance on a HMT, then use low dose Methylmate A and Methylmate B, along with extra B12. |
| Pyroglutamic Acid | Pyroglutamic acid is an intermediate in GSH recycling. There may be too much emphasis on the BHMT pathway, what I call the short cut, of the methylation cycle, or not enough entry into the transulfuration portion when high levels of pyroglutamic are seen. A UAA can be run to assess this balance. Ultimate B may be a help in this regard. Increased gamma glutamyl transferase (GGT) may also generate pyroglutamic acid. This can be due to H. pylori, so rule out H.pylori with testing. Be sure both the long route, the MTR/MTRR pathway, and the short cut, the BHMT pathway, around the cycle are supported, as well as using Ultimate B. You can consider adding low dose GSH. Basic methylation support includes All in One, Phosphatidyl Serine Complex (PS/PE/PC) , DHA and Methylation Support nucleotide blend. Once lithium is shown to be in balance on a HMT, then use low dose Methylmate A and Methylmate B, along with extra B12. |
| Homogentisic Acid | Homogentisic acid is a breakdown product of tyrosine. Check that BH4 levels are sufficient to process tyrosine to dopamine. Look at tyrosine on a UAA and compare that result to the level of dopamine on a NT test. This may indicate whether or not tyrosine is being converted efficiently to dopamine. Without sufficient BH4, excess tyrosine may be forming homogentisic acid rather than dopamine. Decrease Vitamin C, as this may cause a buildup of homogentisic acid. Also, consider that BH4 may need to be supplemented, and if so, support with Royal Jelly if you have NO bee allergies, MTHFR A1298C Liver Support capsules, and BH4. |
| 2-Hydroxyphenylacetic Acid | Processing from phenylalanine can cause increases in 2-hydroxyphenylacetic acid. This can be due to a lack of BH4, or excess phenylalanine or tyrosine. Consider a UAA to look at phenylalanine, tyrosine and the potential need for more BH4. Also, excess aluminum in your system may be impairing BH4 production. Running a HMT and UTM may indicate if your aluminum is high. In addition, aluminum may be sequestered secondary to bacterial issues, so consider a CSA test and GI Test to look at microbial balance. A Neopterin / Biopterin Profile Urine Test should also be considered. If natural support for BH4 is indicated, consider including Royal Jelly if you have NO bee allergies, MTHFR A1298C Liver Support capsules and BH4. |
Looking for a particular supplement or word in this chapter?
Enter your search term here to highlight it throughout the page:
Please be patient as it may take a few moments to search through all of the content.
To search the entire site, not just this chapter, please click the magnifying glass icon
next to ‘Resources’ at the top of the page.
Related Tests to Run
If MMA and FIGLU are high, also consider a UAA to check on methionine, taurine and methylhistidine, as well as a HMT and UEE to check on cobalt and lithium levels. MMA and FIGLU are important indicators of methylation cycle imbalances.
If VMA, HVA and 5 HIAA are all high, consider a NT test to take a closer look at imbalances in neurotransmitters. Look at a HMT and a UEE to check copper, manganese, and molybdenum levels, as these can influence neurotransmitter processing.
If DHPA, quinolinic acid, arabinose, tartaric acid, and/or citramalic acid are high, consider a CSA test and GI Test to determine exactly which microbes are driving up those values.
If beta hydroxy butyric acid or any of the three alpha keto acids are high, or if isovalerylglycine is high, consider a CSA test and GI Test to look at fatty acid breakdown, as ketosis may be an issue. Ketosis may also relate to decreased nutrient uptake, so a UAA to look at overall amino acid levels should be done. If suberic acid is high, then rule out H. pylori.
If homogentisic acid, benzoic acid, and/or hippuric acid are high, consider a Neopterin / Biopterin Profile Urine Test, as well as a UAA, to check phenylalanine, tyrosine, and tryptophan, which may be affected by a lack of BH4. Also, use a HMT and UEE to look at aluminum levels, which can negatively impact BH4 production when homogentisic acid, benzoic acid and/or hippuric acid are high.